Understanding hypermobility, Ehlers–Danlos syndrome, and how strength and movement control help support joint stability.
Many people have flexible joints, and for most, this causes no problems at all. In some cases, however, hypermobility is associated with pain, instability, fatigue, or other symptoms.
Patients, particularly the children and professional dancers I work with weekly, often ask about this after being told they are “very bendy” or after reading information online. Many are highly active people who enjoy movement, and part of my role as an osteopath and clinical Pilates teacher involves helping them understand how flexibility, strength, and joint control interact.
Because hypermobility is common but widely misunderstood, it helps to step back and look at the basics.
What is hypermobility?
Hypermobility means that joints move beyond the range considered typical.
Some people are naturally more flexible because of their genetics, ethnicity, and connective tissue structure. Children and younger adults tend to be more flexible than older adults, and women are often more flexible than men. Hormones that affect connective tissue, including oestrogen and relaxin, may also influence ligament laxity.
Many people with hypermobility have no symptoms. When people are younger, this flexibility can sometimes feel more like a party trick than a problem. Some may have been told as children that they were “double-jointed”. This is not a medical term, and there is no extra joint involved. What people are seeing is simply a joint moving further than usual.
Difficulties tend to arise when flexible joints are also less stable, or when the surrounding muscles have to work harder to control movement.

Hypermobility sits on a spectrum.
- Some people are simply flexible
- Others experience symptomatic hypermobility (Hypermobility Spectrum Disorder)
- At the more complex end are people who meet diagnostic criteria for Ehlers–Danlos syndrome. Understanding where someone sits on this spectrum usually requires proper clinical assessment.
When hypermobility causes symptoms
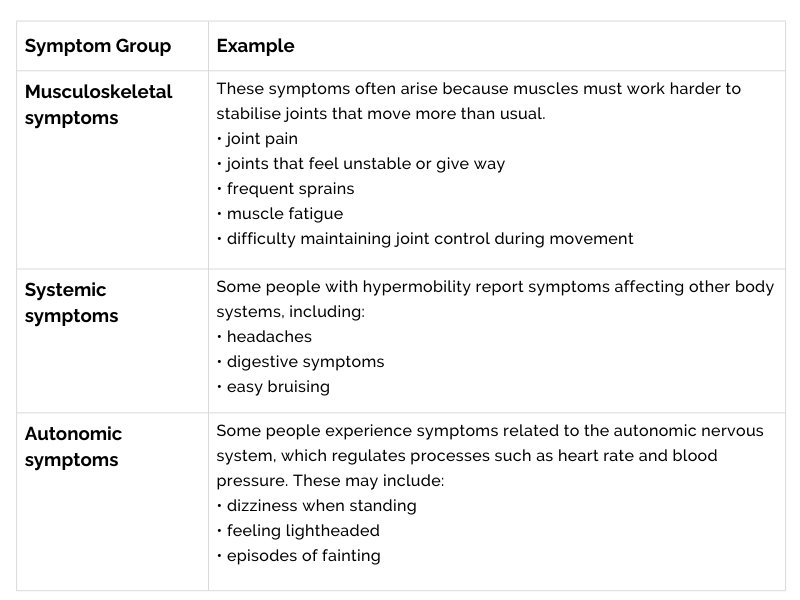
For some people, hypermobility is associated with symptoms affecting different parts of the body.
These vary widely and are not unique to hypermobility, which is why proper clinical assessment matters when symptoms persist or begin to affect daily life.
Hypermobility in different groups
Hypermobility may present differently across age groups.
Children
- Joint hypermobility is common in children, and many have no symptoms.
- When symptoms do occur, they may include:
- Joint pain, often in the legs, after activity or later in the day
- Frequent sprains or minor injuries
- Joints that seem to give way
- Clumsiness or poor coordination
- Fatigue
- Delayed motor skills, such as difficulty with balance
- In many cases, joint flexibility decreases naturally as children grow older.
Women
Hypermobility conditions are diagnosed more often in women.
Some women notice that symptoms fluctuate during the menstrual cycle. Hormonal changes can influence connective tissue and joint stability.
Women with hypermobility sometimes report:
- Increased joint pain around their period
- Heavier or more painful menstrual bleeding
- Pelvic pain
- Symptoms worsening during pregnancy or after childbirth
These symptoms can have many possible causes and should be discussed with an appropriate healthcare professional.
Hypermobility and Ehlers–Danlos syndrome
Ehlers–Danlos syndrome (EDS) is a group of inherited connective tissue disorders.
Connective tissue supports structures throughout the body, including ligaments, tendons, skin, joints, and blood vessels. A key component of connective tissue is collagen, which provides strength and structural support.
In EDS, the way collagen is produced or processed is altered. As a result, tissues may be more elastic, more fragile, or less stable than usual.
Joint hypermobility is relatively common, while EDS itself is considered rare.
Common myths about hypermobility
Myth 1: “I’m double-jointed.”
There is no extra joint involved. The phrase simply describes joints moving beyond their usual range.
Myth 2: “If I feel tight, I need to stretch more.”
Many people with hypermobility feel tight and assume they need more stretching. In reality, this tightness often reflects muscles working hard to stabilise flexible joints. Exercises that improve strength and control are often more helpful than further increasing flexibility, although individual programmes may include both, depending on the situation.
Myth 3: “Flexible joints mean Ehlers–Danlos syndrome.”
Most people with flexible joints do not have Ehlers–Danlos syndrome. Hypermobility is relatively common, while EDS is much rarer.
Myth 4: “Hypermobility is always a problem.”
Many people with hypermobility have no symptoms. Flexibility can even be helpful in activities such as dance or gymnastics.
Myth 5: “There must be a single test.”
Diagnosis is usually based on a combination of history, examination, and clinical criteria. For hypermobile EDS, there is currently no single genetic test.
Assessment and diagnosis
If hypermobility is suspected, clinicians usually begin with a detailed history and physical examination.
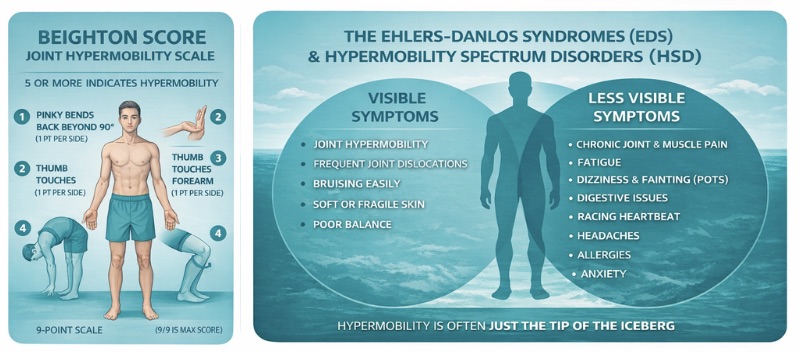
Assessment may include joint flexibility testing, such as the Beighton score; medical and family history; examination of skin and connective tissue features; and genetic testing for some types of EDS. The Beighton score is a screening tool rather than a diagnostic test and should be interpreted alongside symptoms and clinical findings.
For several forms of EDS, there are clear genetic tests. However, hypermobile EDS is currently diagnosed using clinical criteria rather than a specific genetic test.
Management and treatment
There is currently no cure for Ehlers–Danlos syndrome.
Management usually focuses on helping people stay active while improving joint stability and reducing pain. This may include physiotherapy, strengthening and stability exercises, pacing activities, occupational therapy, and pain management, as needed.
Exercise programmes typically focus on improving strength and control rather than increasing flexibility. Most people with hypermobility already have plenty of that.
Many people with hypermobility feel tight and instinctively want to stretch. This often reflects muscles working hard to stabilise flexible joints rather than a true lack of flexibility.
In practice, many people with hypermobility benefit from learning how to improve joint control rather than simply increasing flexibility. As an osteopath and clinical Pilates teacher, I often work with patients to build strength, coordination, and movement awareness so that their joints feel better supported during everyday activities.
With the right approach to strengthening, movement, and pacing, many people with hypermobility can manage their symptoms well and stay active.
When to seek medical advice
Flexible joints alone are common and usually not a cause for concern. However, it can be helpful to seek medical advice if hypermobility is associated with ongoing symptoms or affects daily life.
Consider speaking with a healthcare professional if someone experiences:
- Persistent joint pain
- Joints that frequently give way or dislocate
- Repeated sprains or injuries
- Significant fatigue that affects normal activities
- Dizziness or fainting when standing
- Symptoms that interfere with school, work, exercise, or daily tasks
In children, assessment may be helpful if joint pain regularly limits activity, injuries are frequent, or motor skills such as balance and coordination appear delayed.
A healthcare professional may assess joint flexibility, medical history, and symptoms to determine whether hypermobility is a normal variant or part of a symptomatic condition, such as Hypermobility Spectrum Disorder.
If needed, referral to professionals such as physiotherapists, rheumatologists, or genetic specialists may be considered.
Final thoughts
When hypermobility is associated with pain, instability, or other symptoms, it may be worth further exploration with a healthcare professional.
Understanding the difference between simple flexibility and symptomatic hypermobility helps guide the right approach to activity and joint care.
In clinical practice, this often involves helping people understand how their joints move and how strength, coordination, and sensible load management can support long-term joint health. Approaches such as osteopathic treatment and carefully progressed clinical Pilates exercises can help people remain active and confident in their movement.
Reliable places to learn more
Author
Sandie Ennis is an osteopath, Pilates teacher and clinical educator working in Dulwich and Central London. Her work focuses on hands-on treatment, therapeutic movement, and rehabilitation to help people maintain strength, mobility, and independence throughout life.