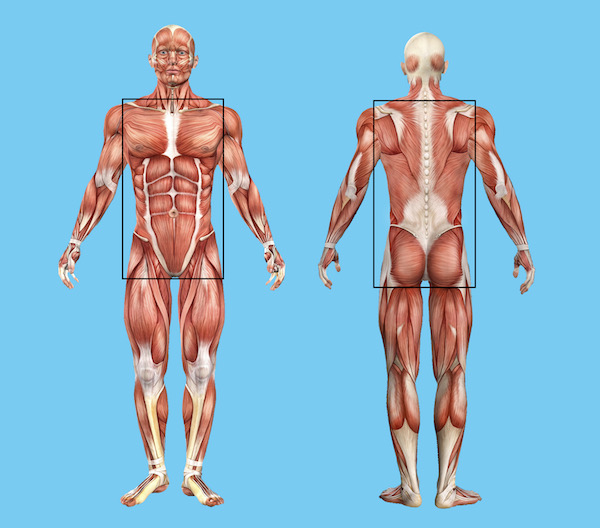
The “core” is scientifically called the lumbopelvic-hip complex (LPHC). It’s everything our head, arms and legs attach too, the torso or trunk of the body. Most often its acts as a stabiliser and force transfer, yet people focus on training it in isolation as a prime mover, with exercises like sit-ups, crunches, and planks. If that all you do, you are missing out on a significant aspect function and more efficient movement.
In reality, most of us living in the developed world, need to add back the functional * closed chain movements missing from our daily lives. Hence the need to exercise in the first place, think of some aspects of exercise as a supplement to get the nutrients missing from your daily diet: squats, twists and overhead arm reaches.
Torso (core) stability has several components: motor control, strength, flexibility, function, and endurance, all of which should eventually be dynamic rather than static - sit-ups and planking. Motor control and function are the essential elements that provide the foundation for the remaining three.
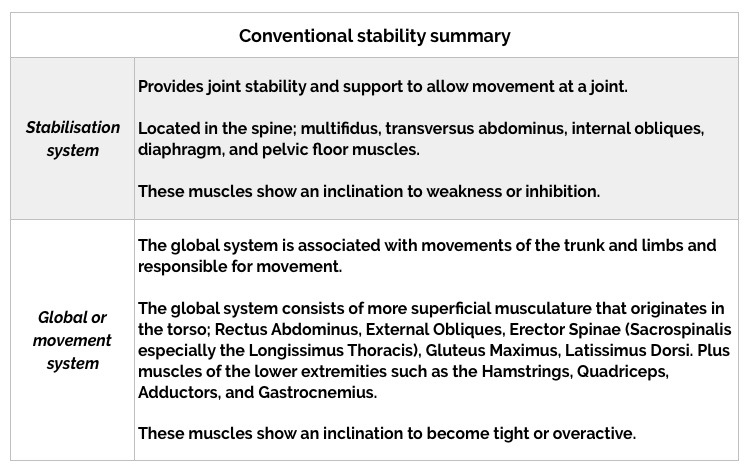
Conventional approaches view muscles as having isolated actions and functions and propose that two distinct, interdependent muscular systems enable our bodies to maintain proper stabilisation and ensure efficient distribution of forces for the production of movement.
Muscles located more centrally to the spine are known as part of the stabilisation system and provide intersegmental stability, or vertebrae to vertebrae stability whereas muscles further away from the spine, are known as the global or movement system, and support the spine as a whole.
Training programs should be functional if at all possible, by that I mean movements based on real-life moves used in daily tasks at home, at work or in sports. They should include rotational movements, and pushing, pulling, lunging, and squatting. Plus multi-planar, multi-joint actions that place a demand on the body’s whole torso musculature, for example, squats with arm or head movement or with a load.
Where to start if you need or want to work on your trunk stabilisation (core)
Well, it depends (sorry, its standard osteopathic answer) ), some people need to work on releasing tight muscles and get flexible first while others need to begin with motor control, and another strength training is their best way forward. For most of the people I work with; patients with multifactorial often complex chronic presentations, and fear of moving. I find motor control is the most useful place to start because it gives them confidence with static movements, and reduces their perception of motion (movement) and mobility equalling pain.
There is no evidence that this approach protects the spine and surrounding musculature from injury, and I tell them that too, but in my twenty years as a movement professional. Plus 26 years managing my own complex and significant spinal injury it offers an excellent place to start with the people who reach out to me, usually because I have some lived experience.

Once the initial phase is working well, it’s time to move on to dynamic movements. It’s essential to effectively and efficiently produce and transfer force during progressive, dynamic movements while maintaining torso stability. Without motor control, the other components are not helpful. For example, lifting a bag of groceries from the boot of a car, or the wriggling grumpy toddler from their car seat. So making exercise functional while keeping them feeling stable and safe becomes a creative challenge that may involve some trickery and skill.
Regardless of the specific exercise or movements utilised, training programs should have patient/client/specific goals and be progressive. Slow, controlled, elementary exercises such as isometric transversus abdominis exercises and Pilates pelvic curls (tilts) are often the best starting level depending on the person’s level of pain, strength, and control. Or their level of anxiety and fear avoidance. When they can perform these exercises well and can maintain a regular breathing pattern, they may progress - moving on from a single plane to multi-plane movements, from isometric to concentric and eccentric contractions.
Multi-planar stability activities with one side of the body working independently of the other, are the most functional because it offers the dynamic movement of the body in three dimensions simultaneously. Activities such as running require controlling ground reaction forces, delivering propulsion forces, and the dynamic stabile movement of the body. Except, most people in pain or with chronic problems are not going to running anywhere, so what are you going to do with them? Pilates leg slides, prone arm or leg raises, as preparation for the joys of running later, if they can and choose to run.

What else? Rehabilitation therapists and movement coaches need to get people to work with variations in the speed of movements: slow to fast. Not an element used much in classic Pilates, but hopefully one does not live life in one gear, so modern adaptions of the method [Pilates] have incorporated this.
Where to next? Isolated movements may be enough for targeting specific muscles, but the gains may not carry over into everyday life. Plus I don’t think muscle, but movement and joints. So starting without resistance and building to resisted movements is an option, adding limb movement another, and vary from lying-down positions to sitting and standing best.

Be patient; movement re-education exercises should progress only when the patient/client/you feel secure. Can maintain spinal stability with regular calm breathing - to reduce stress hormones. This may take some time, your kindness and repetition, lots of repetition, especially in people with persistent pain histories, complex trauma or comorbidities, because they need to feel free from perceived or real danger.
While you are supporting them to explore the opportunities, risks, and benefits of new movements in unfamiliar positions. Oh, and make it enjoyable and fun, it’s going to be work, but in my opinion, too much of rehabilitation journey is tedious and boring, and it doesn’t have to be, make it playful if you can, ask them how if you can’t.
*Closed chain exercises are those performed where the hand or foot (extremity) is fixed and cannot move, and remains in constant contact, usually with the ground or the base of an exercise machine.